Agreement of Release and Waiver of Liability
I Hereby agree to the following:That I am participating in lifestyle and fitness consultation and programs or workshops by Body By Sandra Nelson L.L.C. I will receive information about lifestyle(Meal coach) and fitness programs that many require physical exertion,which I may be strenuous and may cause injury, I am fully aware of risks and hazards involved.
1)I understand that it is my responsibility to consult with a physician prior to and regarding my participationin the lifestyle and fitness programs,classes or workshops.
2)I have either had a physical examination and been given permission to participate in physical activity without the approval of a physician
3)I do hereby assume all responsibility for my participation and activities with gym equipment and machinery in my activities.
4)Body by Sandra Nelson L.L.C. in no way intended to diagnose,treat,cure or prevent any disease through any services or programs provided by Body by Sandra Nelson L.L.C.
5)I agree to assume full responsibility for any risks,injury,or damages known and unknown,which might occur as a result of participating in the programs.
6)I knowingly,voluntarily and expressly waive any claim I may have against Body By Sandra Nelson L.L.C. for injury or damages that I may sustain as a result of participating in the programs.
7)I, my heirs or legal representatives forever release,waive,discharge and covenant not to sue Body by Sandy Nelson L.L.C. for any injury or death caused by their negligence or other acts.
I have read the above and release and waiver of liability and fully understand it's contents. I voluntarily agree to the terms and conditions stated above.
Date
Signature of participant/or checked online
**Cancellation Policy 24 hour cancellation must be received online or session will be charged to account.
Meal Coach Waiver
1. I fully understand that Sandra Nelson ( Body by Sandra Nelson L.L.C.) is a Meal Coach …This is only a recommendation based on my education and of experience working with all of my personal clients.
2. I fully understand that Sandra is NOT a Registered Dietician ,nutritionist ,or licensed nutritionist and does not diagnose,assess, treat or cure any disease or pathological medical condition, or prescribe any medication. I am not here for medical diagnoses or treatment, but for meal coaching. I understand that no claims are made for results of dietary/nutritional suggestions .
3. I have solicited the services of Sandra in good faith, exercising my free will and following the dictates of my own conscience, which allows me to select what I understand is most beneficial to my health.
4. I presently seek advice, opinions or points of view and /or programs within the scope of Sandra’s practice.
5. I fully understand that Sandra is in no way encouraging me to discon- tinue or disregard any medication or medical advice given by my primary care physician or any other medical professional.
6. I hereby acknowledge that I have read and understand this document in its entirety. Client Signature________________________________Date____________
Or Box checked
THANK YOU FOR YOUR TIME.
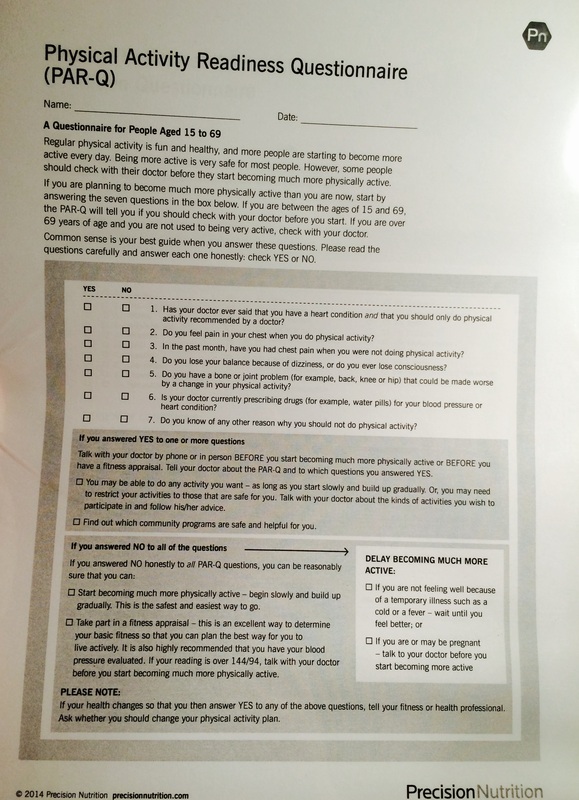
Please take a moment to read through the Par Q and notes guidelines of recomendations to exercise or seek medical attention.
I Hereby agree to the following:That I am participating in lifestyle and fitness consultation and programs or workshops by Body By Sandra Nelson L.L.C. I will receive information about lifestyle(Meal coach) and fitness programs that many require physical exertion,which I may be strenuous and may cause injury, I am fully aware of risks and hazards involved.
1)I understand that it is my responsibility to consult with a physician prior to and regarding my participationin the lifestyle and fitness programs,classes or workshops.
2)I have either had a physical examination and been given permission to participate in physical activity without the approval of a physician
3)I do hereby assume all responsibility for my participation and activities with gym equipment and machinery in my activities.
4)Body by Sandra Nelson L.L.C. in no way intended to diagnose,treat,cure or prevent any disease through any services or programs provided by Body by Sandra Nelson L.L.C.
5)I agree to assume full responsibility for any risks,injury,or damages known and unknown,which might occur as a result of participating in the programs.
6)I knowingly,voluntarily and expressly waive any claim I may have against Body By Sandra Nelson L.L.C. for injury or damages that I may sustain as a result of participating in the programs.
7)I, my heirs or legal representatives forever release,waive,discharge and covenant not to sue Body by Sandy Nelson L.L.C. for any injury or death caused by their negligence or other acts.
I have read the above and release and waiver of liability and fully understand it's contents. I voluntarily agree to the terms and conditions stated above.
Date
Signature of participant/or checked online
**Cancellation Policy 24 hour cancellation must be received online or session will be charged to account.
Meal Coach Waiver
1. I fully understand that Sandra Nelson ( Body by Sandra Nelson L.L.C.) is a Meal Coach …This is only a recommendation based on my education and of experience working with all of my personal clients.
2. I fully understand that Sandra is NOT a Registered Dietician ,nutritionist ,or licensed nutritionist and does not diagnose,assess, treat or cure any disease or pathological medical condition, or prescribe any medication. I am not here for medical diagnoses or treatment, but for meal coaching. I understand that no claims are made for results of dietary/nutritional suggestions .
3. I have solicited the services of Sandra in good faith, exercising my free will and following the dictates of my own conscience, which allows me to select what I understand is most beneficial to my health.
4. I presently seek advice, opinions or points of view and /or programs within the scope of Sandra’s practice.
5. I fully understand that Sandra is in no way encouraging me to discon- tinue or disregard any medication or medical advice given by my primary care physician or any other medical professional.
6. I hereby acknowledge that I have read and understand this document in its entirety. Client Signature________________________________Date____________
Or Box checked
THANK YOU FOR YOUR TIME.
Please take a moment to read through the Par Q and notes guidelines of recomendations to exercise or seek medical attention.